
By Dr Erin Nesbitt-Hawes – Endometriosis Australia’s Clinical Advisory Committee
Laparoscopy or keyhole surgery has been the main surgical approach to the treatment of endometriosis since it was developed in the early 1980’s. There are a number of laparoscopic techniques that are used to remove the disease and there are pros and cons of each. Laparoscopy in the treatment of endometriosis has the benefit of being both diagnostic (to identify the cause of pelvic pain) and therapeutic (to treat the cause of pelvic pain).
Ablation of endometriosis is performed using heat energy to destroy the abnormal cells where they lie. At the time of laparoscopy, endometriosis is identified visually and then an instrument using an electrical current to produce heat energy is used to vaporise or burn the affected tissues. There are a number of disadvantages to this approach including the limitations of not obtaining a specimen for pathological diagnosis. As mentioned above, laparoscopy is a diagnostic intervention however if pathology is not sent off for review the diagnosis of endometriosis relies on the naked eye of the surgeon alone (something which is dependent on the skill and experience of the surgeon and is not as accurate as pathology).
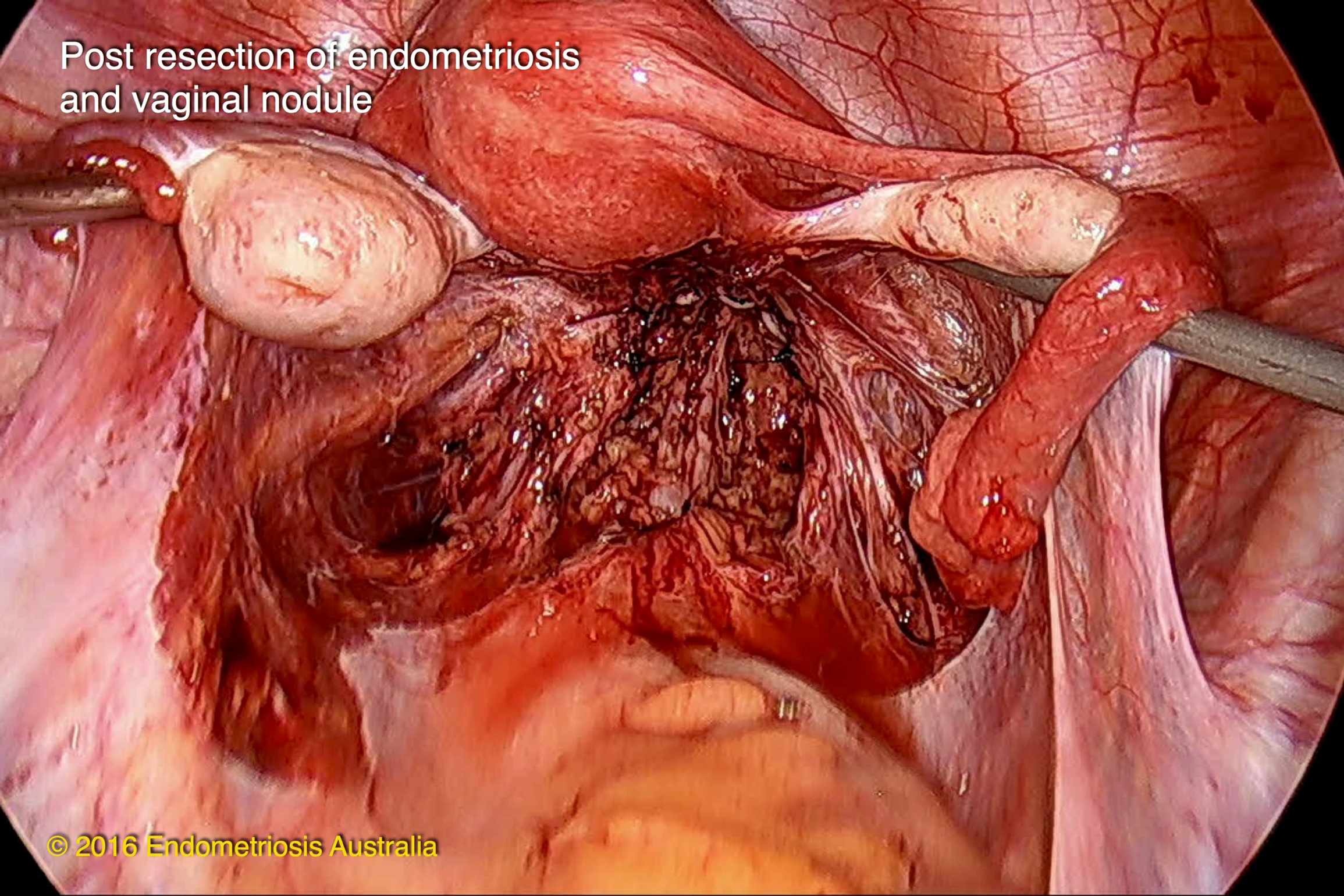
Excision of endometriosis is a technique where the abnormal cells are removed from the affected organs. Again heat energy is often used for this purpose, but unlike ablation the energy when used for excision acts like a knife through the tissue. As the abnormal tissue is removed without affecting the cells it has the benefit of being able to be sent for pathological diagnosis.
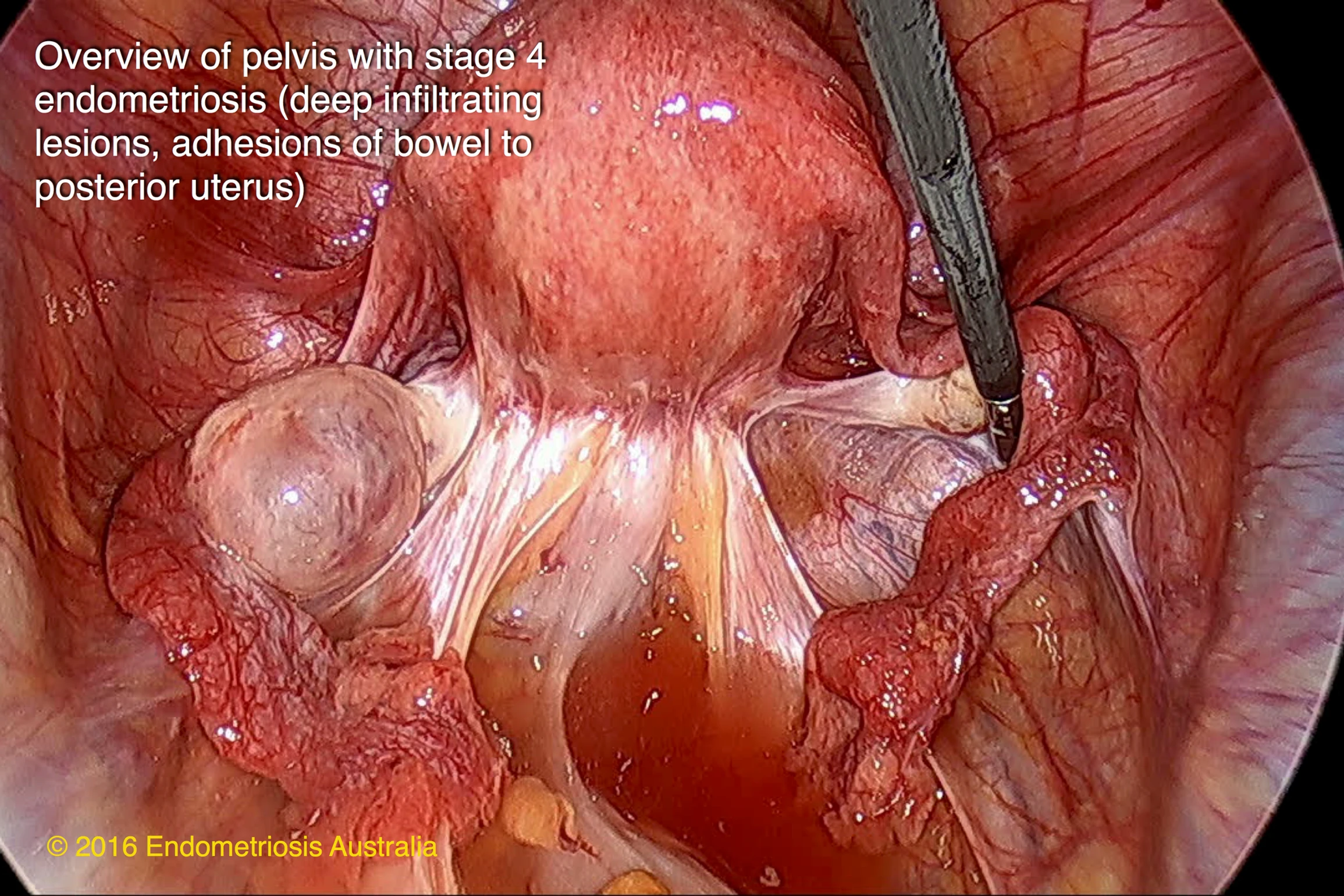
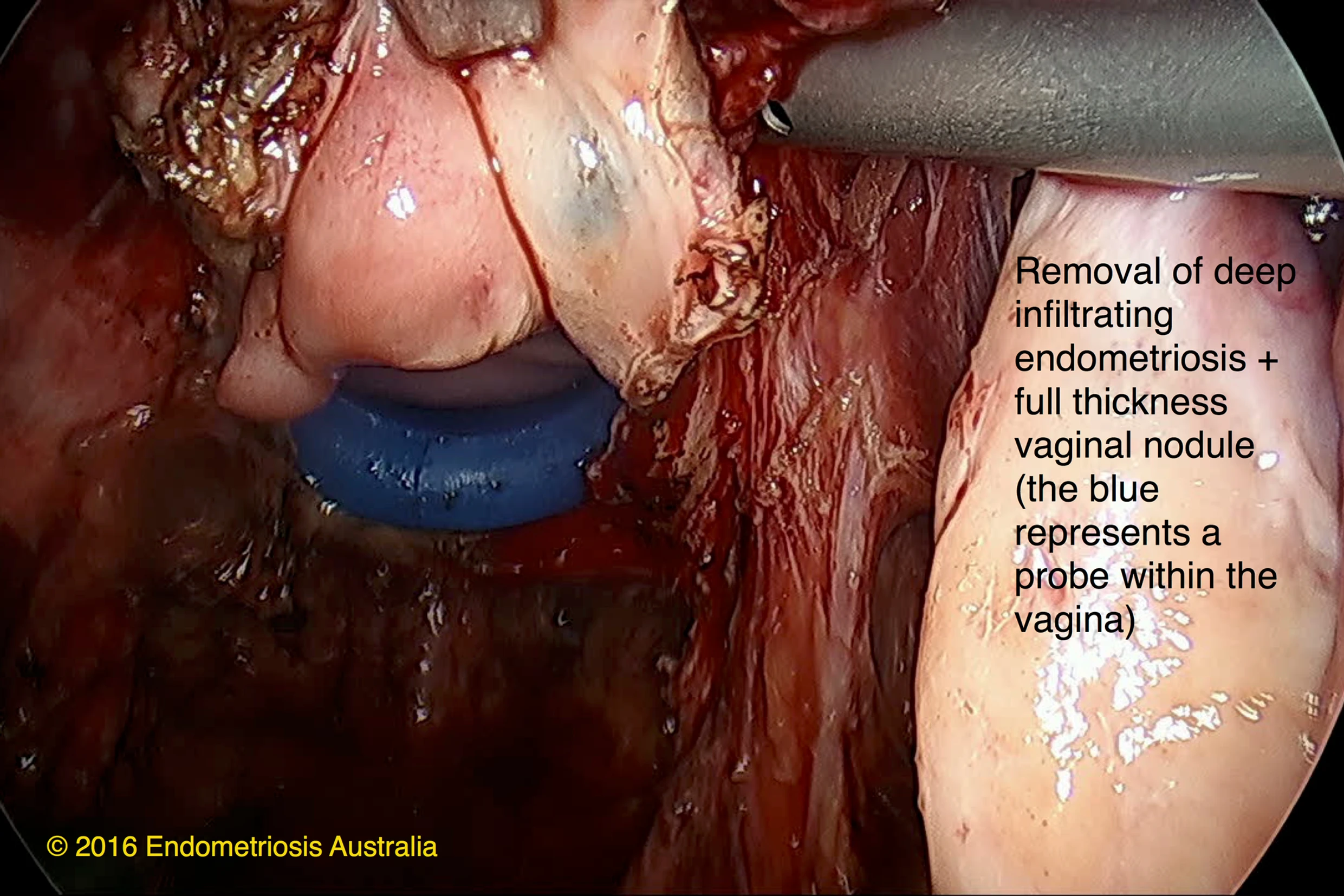
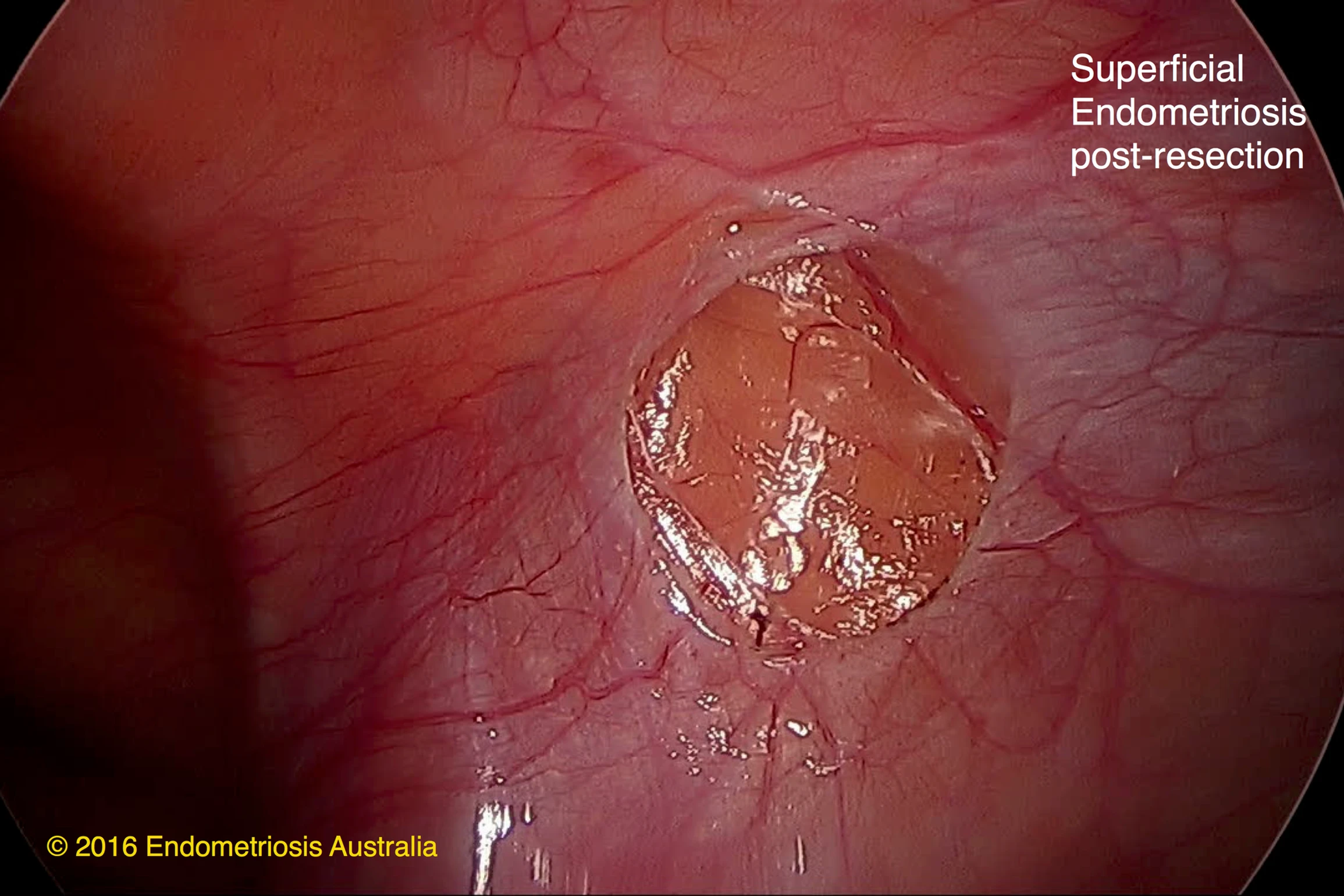
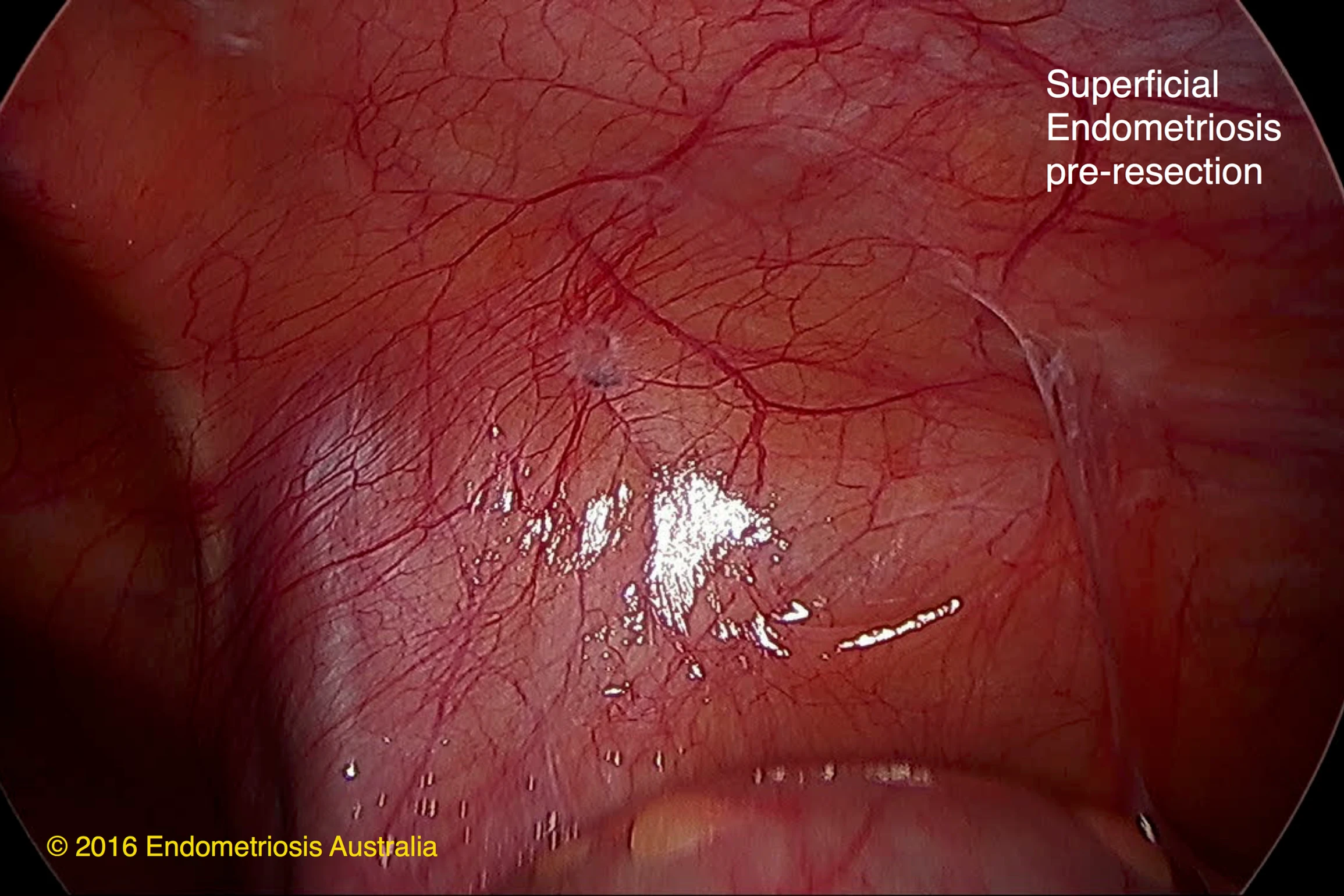
Endometriosis often lies on an internal covering layer of tissue called the peritoneum. The peritoneum is like a ‘glad-wrap’ layer over the organs. The excision technique allows this layer to be peeled back, taking the endometriosis with it. Deep infiltrating deposits require more removal than just peeling, but with the excision technique it is possible to clearly identify the demarcation between healthy normal and abnormal tissues allowing complete resection. Ablation on the other hand only allows the superficial disease to be treated. This can mean that an underlying ‘iceberg’ of endometriosis is not diagnosed or treated effectively. Research into the difference between excision and ablation shows that for the symptom of painful intercourse (dyspareunia) excision is superior.
A further difference between excision and ablation of endometriosis relates to the potential for complications. As excision uses more judicious use of energy to cut the tissues rather than burning, the risk of thermal spread of the heat energy is less meaning that vital organs such as the ureters, bowel and bladder are less likely to be inadvertently injured in the process. Having said this, it is important to realise that either technique has the potential to cause injury to associated organs. Surgeon skill and experience as well as specialisation in removal of endometriosis are all factors to consider when choosing the surgeon who performs your operation.Lastly, robotic assisted surgery is a newer frontier in gynaecology and is being used for the resection of endometriosis in some cases. This is not surgery where are walking, talking robot takes the place of your surgeon, rather the instruments that are inserted at the time of laparoscopy are attached to the robot which is then externally controlled by the surgeon. The benefits of this type of surgery are partly for the surgeon, allowing them to sit down at a console rather than standing for hours in potentially awkward positions and to see in three dimensions. From a surgical point of view, certain movements are easier, such as putting in internal stitches due to the wide range of motion of the robotic instruments compared with traditional laparoscopic instruments.
Robotic assisted surgery has still not been proven to have an increased benefit over standard laparoscopic techniques for most benign gynaecology indications. However certain procedures which require more precision may benefit. This includes the treatment of gynaecological cancers with improved removal of lymph nodes. It may be that for severe stage 4 endometriosis involving bowel or overlying the ureters that the robot proves to be more beneficial but the evidence for this is still lacking. Currently due to significant expense of the disposable instruments required to operate the robot this is not a surgical option generally offered in Australia and it is not possible to justify the cost at this stage without the associated evidence to prove its superiority.
Knowledge is king and research into the best way to surgically treat endometriosis is ongoing as part of the ambition to discover more about the best ways to help women with this condition.